Egg Freezing: 8-easy steps
STEP ONE: PHYSICIAN INITIAL CONSULTATION
Each patient is seen by Dr. Vincent Brandeis, a board board-certified reproductive endocrinologist.
At the first visit (in office or televisit), there will be a detailed medical and gyn history.
A transvaginal sonogram is done to visualize the uterus and ovary and determine if there are ovarian cysts, fibroids, or other gyn issues that should be addressed before starting the process of egg freezing.
STEP TWO: FERTILITY ASSESSMENT - AMH & FOLLICLE COUNT
To determine the number of eggs present and the quality of the eggs:
a. AMH – Blood will be drawn to determine the level of AMH.
b. Antral Follicle Count – Ultrasound study to assess the number of egg cells available.
c. Baseline Hormone – Estradiol, FSH, LH, Progesterone, during the first five days of menstrual cycle.
d. Reproductive health test – Thyroid Panel, Prolactin, DHEA, CA-125. Free + total Testosterone, Insulin, Hemoglobin A1C
STEP THREE: POST-FERTILITY ASSESSMENT MEETING - REVIEW TEST RESULTS
A one-on-one meeting with Dr. Vincent Brandeis to discuss in detail the results of your fertility assessment.
This comprehensive evaluation is used to provide a realistic idea of how many eggs are likely to be retrieved and the chances of these eggs to be fertilized after they are thawed.
Atreatment plan to discuss the medications and doses that will be needed to stimulate your egg cells.
We individualize the stimulation protocol base upon
Age, Height and Weight (BMI) and the results of your AMH and antral follicle count.
It is also helpful to review the results of you past fertility cycles
STEP FOUR: DETERMINE STIMULATION PROTOCOL
Meet with your clinic coordinator and/or fertility expert to discuss the specific timing of your stimulation cycle.
At that session, we will discuss again the medications to be use for egg/follicle stimulation.
We will also discuss how to administer these medications, what happens during office visits for vaginal sonograms and blood drawing for hormonal levels, how the eggs are retrieved, how the eggs will be frozen and stored.
STEP FIVE: STIMULATION OF EGG CELLS
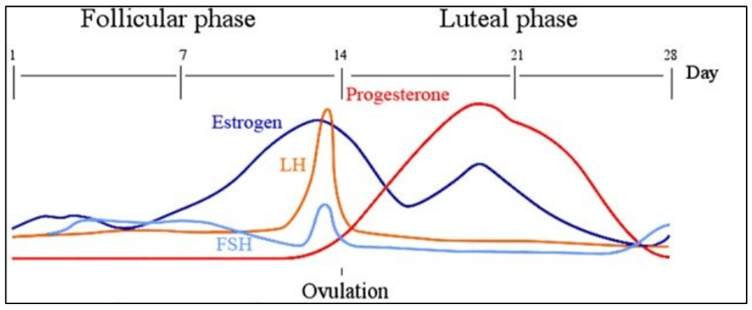
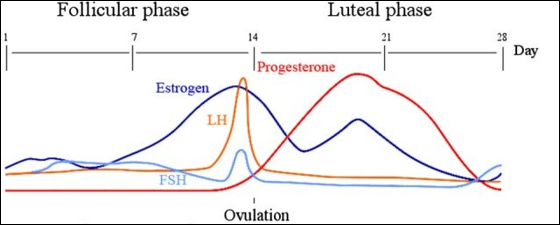
 During a natural menstrual cycle, the pituitary gland in the brain produces FSH and LH hormones that stimulates the growth of one or several egg cells in the ovary.
During a natural menstrual cycle, the pituitary gland in the brain produces FSH and LH hormones that stimulates the growth of one or several egg cells in the ovary.
As the egg cells grow, there will be a increase production of Estradiol from the follicles (tiny sacs in which the egg cell grow until they are retrieved)
The medications we administer are:
- Gonal-F – FSH only
- Menopur – combination of FSH and LH
- Low-dose hCG – a medication that closely resembles natural LH
- Cetrotide – an “anti-gonadotropin-releasing hormone” used to prevent ovulation (the release of an egg from the ovary) during the 10 days of stimulation
Our sincere caring goal – stimulate as many mature eggs as possible – hopefully 10-20 mature eggs depending upon your fertility potential.
We prefer to monitor you at least every other day from days 1 to 6, and everyday 7, 8, 9, 10.
Monitoring includes: blood test (estradiol), vaginal sonogram (number/size of follicles)
Every patient has a different response to these medications and each patient has a different response cycle-to-cycle.
Monitoring the Rise in Estradiol in 10 Days of Stimulation
Usually, the estradiol level at the start of the cycle is 30 to 70 pg per mL.
Estradiol level rises from 300 to 500 from one follicle in a natural cycle
and up to or over 3,000 with stimulation on day of retrieval.
The reason why the estradiol level rises so high is that instead of one follicle developing under the influence of natural low-levels of FSH and LH, we now have 30 follicles developing under the influence of injectable high-dose FSH and LH.
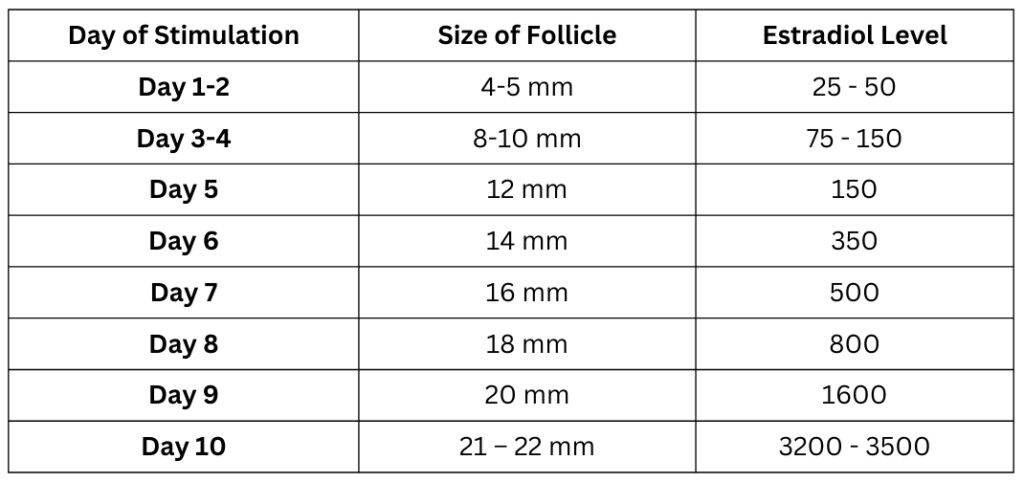
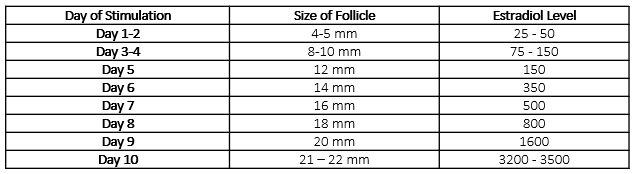
Monitoring the Size of the Follicles in 10 days of Stimulation
Day 1 and 2 of menstrualcycle, the size of the follicle/s is usually 4-5 millimeters–about the size of the pencil eraser head.
The follicle containing the egg will start to increase in size after about 3-4 days of stimulation.
Typically, after the follicle starts to increase in size from 4 mm in the first few days,
The follicle will increase in size, 2 mm a day. – as seen below
Table 1: A typical response in follicle size and estradiol level to fertility medications during stimulation for egg freezing
STEP SIX: EGG RETRIEVAL (OOCYTE RETRIEVAL)
It is necessary to fast the night before the retrieval because the procedure is done with light intravenous anesthesia sedation to ensure that your retrieval will be painless and you will be comfortable both during and after the procedure.
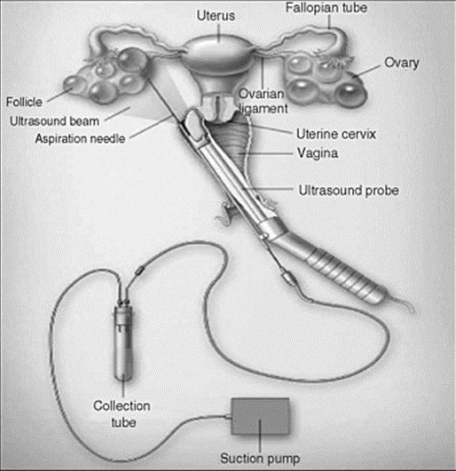
The retrieval is accomplished using the same type of ultrasound machine that is used for your daily monitoring.
A needle guide is attached to the vaginal ultrasound probe through which a thin special aspiration needle can be inserted through the opening into the needle guide.
Once you are fully asleep, the vaginal probe with the needle guide is gently introduced into the vagina and then the needle is inserted into the guide and passes through the vaginal wall to reach each ovary.
Using ultrasound guidance, the follicles in each ovary can be easily identified. The fluid in each follicle contains the egg cell and this fluid with its egg cell is gently removed with very mild suction from the ovary into a special test tube – which is then handed to the laboratory technician.
Egg retrieval itself takes about 20 minutes. Most patients are awake within 20-30 minutes and usually able to go home within an hour. As a precaution, most patients are given several days of antibiotics to decrease the likelihood of an infection which is extremely uncommon.
On the day of the egg retrieval, please have a family member or friend available to bring you home after the procedure.
STEP SEVEN: CRYOPRESERVATION IN THE LABORATORY
1. Oocyte Assessment and Selection
- In the IVF laboratory, embryologists examine the retrieved eggs under a microscope.
- Only mature oocytes at metaphase II (MII stage) are selected for freezing. Immature or abnormal eggs are excluded.
2. Equilibration with Cryoprotectants
- Oocytes are highly sensitive to ice crystal formation, so cryoprotectants are used to dehydrate and protect the cells.
- Two types of cryoprotectants are used:
- Permeating cryoprotectants (e.g., ethylene glycol, DMSO): Enter the cell and prevent intracellular ice formation.
- Non-permeating cryoprotectants (e.g., sucrose): Help draw water out of the cell to reduce volume and osmotic stress.
- The oocyte is first placed in an equilibration solution with low concentrations of permeating cryoprotectants. This allows gradual dehydration and cell adaptation.
3. Vitrification Solution and Rapid Cooling
- The oocyte is then moved to a high-concentration vitrification solution (rich in cryoprotectants) for less than a minute to complete dehydration and prepare for vitrification.
- The egg is loaded on a special carrier device (e.g., Cryotop, Cryoloop, or HSV straw).
- Immediately, the loaded carrier is plunged directly into liquid nitrogen at –196°C.
This process happens very quickly—the egg turns into a glass-like solid without forming ice crystals. This is the key feature of vitrification and what makes it safer and more effective than slow freezing.
STEP EIGHT: LONG-TERM STORAGE OF OUR OOCYTES AT REPROLAB
We transfer all frozen oocytes to Reprolab located at 332 E 30th St, New York, NY 10016.
1. What process is used to transfer the frozen egg cells
After vitrification, oocytes are:
- Loaded onto specialized straws or vials, we use the Cryotop.
- The Cryotop immediately submerged into liquid nitrogen (LN₂) to ensure ultra-rapid cooling and solidification without ice crystal formation.
2. Placement into Cryovials or Protective Sleeves
- The cryovial is:
- Properly sealed
- Labeled clearly with patient ID, date, type of cell (MII oocytes), and unique identifiers.
3. Transfer to Long-Term Cryogenic Storage Tanks
The vitrified oocytes are then transferred as follows:
A. Use of Canisters and Canes
- Cryovials is placed inside metal canes (stainless steel).
- These canes are slotted vertically into canisters—cylindrical baskets suspended in the storage tank.
- Each cane/canister is labeled and indexed according to a cryostorage inventory system.
B. Insertion into Storage Tank
- The canister is submerged entirely into the liquid nitrogen phase of the cryogenic tank (–196°C).
4. Ongoing Storage Conditions
- Tanks are equipped with:
- Temperature probes
- Level sensors
- 24/7 alarm systems to detect loss of liquid nitrogen in the tank.
